First author: Federica Ilardi
Department of Advanced Biomedical Sciences, Federico II University Hospital, Via S. Pansini, 5, 80131 Napoli NA, Italy
Dobutamine stress echocardiography (DSE) is a sensitive diagnostic tool to detect inducible ischemia, thanks to its good diagnostic accuracy. However, it remains a subjective method, limited by operators experience on image acquisition and interpretation. Moreover, the detection of myocardial ischemia during DSE seems to be even more challenging in the presence of pre-existing wall motion abnormalities.
Nowadays, speckle tracking allows an objective quantification of regional wall function. To date, few reports have described the ability of speckle tracking to detect myocardial ischemia during DSE and mostly in patients without previous regional wall motion abnormalities. Considering the exclusion of patients with previous history of coronary artery disease from these studies, their results cannot be extended to this subset of patients.
In the present study, we aimed to investigate the feasibility and accuracy of global (GLS) and regional longitudinal strain (RLS) during DSE to detect significant coronary stenosis (SCS), in both patients with and without previous wall motion abnormalities.
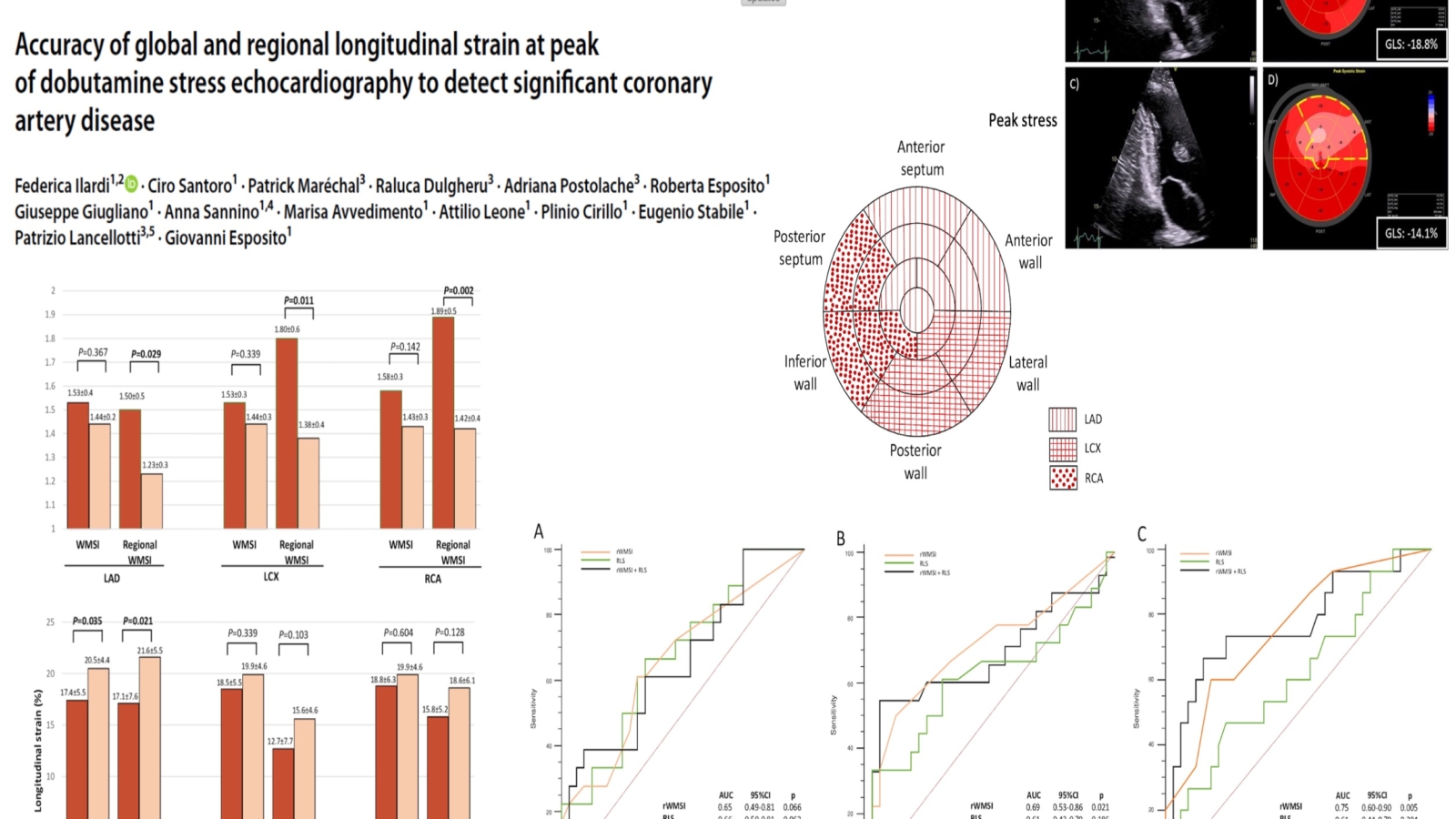
We conducted a prospective, observational, multicenter study, including 88 patients undergoing DSE for suspected CAD. Patients with negative DSE (n=33), suboptimal RLS (n=2) and that refused consent (n=3), were excluded from further analysis. The remaining 50 patients (82% males, mean age 66.3±8.2 years) with positive DSE underwent subsequent invasive coronary angiography (CA). Besides visual regional wall motion score index (WMSI), GLS and RLS were determined at rest and at peak stress by a dedicated software (Automated Function Imaging) incorporated in a quoad-screen of the echo machine and activated by automatic quantification. Obstructive CAD was defined as >70% stenosis or intermediate stenosis combined with fractional flow reserve <0.80.
We found that speckle tracking can be performed during DSE, allowing a correct and almost complete analysis of myocardial deformation, at every stages of stress protocol (the feasibility of RLS was 96% in the pooled population). Fifteen patients did not show significant coronary artery stenosis whereas obstructive CAD was detected in 35 patients. At peak stress, both GLS reduction (p=0.037) and WMSI worsening (p=0.04) showed significant agreement with coronary angiography for detecting SCS. When single lesion was considered, peak stress GLS and LAD RLS were lower in the obstructed LAD regions than in normo-perfused territories (17.4±5.5 vs 20.5±4.4%, p=0.03; 17.1±7.6 vs 21.6±5.5%, p<0.02, respectively). Furthermore, the addition of RLS to regional WMSI was able to improve accuracy in LAD SCS prediction (AUC 0.68, p=0.037). Conversely, in presence of LCX or RCA SCS, longitudinal strain was less accurate than WMSI at peak stress.
This incremental value of strain imaging at DSE peak could represent an additional tool in reducing false negative results obtained by visual assessment, especially in patients with suspected LAD disease. LAD is usually the largest of the 3 epicardial coronary artery and subtends about 50% of the LV myocardial mass. The presence of significant LAD disease has been associated with worse prognosis than SCS involving other coronary arteries. Thus, given the extent and functional relevance of the myocardial territories supplied by LAD coronary artery, a properly and timely detection of LAD stenosis represents an appealing task. Moreover, the incremental value of GLS and RLS in the detection of LAD SCS seems to be even more useful in patients with previous wall motion abnormalities, in whom the identification of residual and/or new areas of ischemia is even more challenging.
In conclusion, AFI-based strain quantitative analysis appears to be highly feasible during DSE and more accurate than the visual wall motion assessment for the detection of myocardial ischemia in presence of LAD. Conversely, strain accuracy is suboptimal in patients with LCX and RCA stenosis, possibly due to scarce visualization of myocardial segments perfused by these two arteries and/or to perfusion territory overlap. Future multicenter study on larger population sample size are needed to test the usefulness of strain imaging during DSE.
Read More: https://pubmed.ncbi.nlm.nih.gov/33433744/